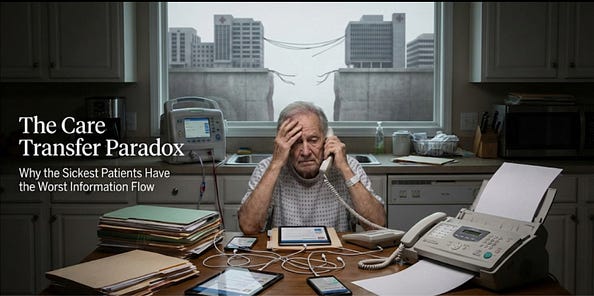
The Care Transfer Paradox
by Serelora
This article was originally published on Medium.
Read full article on MediumWhy the Sickest Patients Have the Worst Information Flow
By Luis Cisneros, CEO | Serelora
There is something curious about modern healthcare that we have all quietly agreed not to notice. The sicker you become, the harder it gets for your information to travel between the people trying to help you.
This is not a bug in the system. It is the system.
A healthy person can pull up their cholesterol numbers on a smartphone app while waiting for coffee. A patient with end-stage renal disease, navigating a forty-step pathway toward a kidney transplant that could add a decade to their life, cannot get a cardiac clearance faxed to the transplant center before the evaluation window closes. A cancer patient moving between oncology, radiology, and palliative care discovers that each department operates as if the others do not exist. A heart failure patient discharged from the hospital arrives at their follow-up appointment only to learn that the cardiologist has no record of what happened during the admission.
We might call this the Care Transfer Paradox. And by care transfer, I mean something broader than data exchange. I mean the movement of records, decisions, and accountability across people and sites of care. The full handoff that should happen when a patient moves from one context to another. The complexity that generates the need for this coordination is the same complexity that defeats it. The patients who need information to move fastest are precisely the patients for whom it moves slowest. Healthcare has somehow arranged itself such that the most resource-intensive, highest-stakes clinical scenarios are also the ones most likely to be derailed by a fax machine, a missing form, or an authorization that expired while sitting in someone’s inbox.
The temptation, of course, is to treat this as a technical problem. Interoperability standards. Better APIs. Smarter software. If we could just connect the systems, the thinking goes, data would flow and coordination would follow.
This framing is seductive and almost entirely wrong.
The bottleneck is not capability. The pipes exist. FHIR protocols work. Patient-directed APIs have been built. The bottleneck is governance, incentives, and liability posture. American healthcare did not stumble into fragmented information systems the way one stumbles into a poorly lit room. It built them deliberately, over decades, in response to institutional priorities that had nothing to do with patient coordination and everything to do with institutional protection.
Consider HIPAA. The regulation explicitly permits sharing of protected health information for treatment, payment, and healthcare operations without patient authorization. The legal framework allows for coordination. Yet institutions routinely behave as if HIPAA forbids it, because risk management teams have concluded that the safest interpretation is the most restrictive one, and because no one gets fired for refusing to share a record. The compliance officer’s reflex is not “how do we share this safely?” but “what is our liability exposure if we share at all?” The regulation meant to protect the patient has been operationalized, through institutional risk aversion, as the justification for excluding the patient from their own care.
Protection becomes exclusion. This is the first inversion, and it is far from the last.
The Patient as Makeshift Infrastructure
Let us be concrete for a moment, because abstraction makes it too easy to look away.
Consider kidney disease. A patient begins hemodialysis. Three times per week, four hours per session, they are tethered to a machine that performs the blood filtration their kidneys can no longer manage. They are exhausted. They are often cognitively impaired in ways the medical literature describes with clinical detachment but which feel, to the patient, like trying to think through wet concrete. They are told, somewhere between medication adjustments and dietary lectures, that transplantation is an option, that it could restore near-normal physiology, that survival rates favor transplant over dialysis by every available measure.
What happens next should be straightforward. Referral to a transplant center, evaluation, testing, waitlisting, surgery, recovery, life.
What actually happens is a labyrinth designed by someone who has never had to navigate it while chronically ill. The dialysis center has records of sessions and lab values in one system. The nephrologist has consultation notes in another. The cardiologist who performed the required stress test has results in a third. The primary care physician has vaccination history in a fourth. The patient is told to “coordinate” the transfer of all this information to the transplant center.
Coordinate. As if they were a project manager with a Gantt chart and a functioning email system. As if they were not spending twelve hours per week hooked to a machine, managing dietary restrictions, coping with fatigue that makes grocery shopping feel like summiting Everest, and slowly dying.
The patient becomes the infrastructure. They become the human router through which data packets must travel because the institutions refuse to talk to each other directly. And they are expected to perform this role while their body is actively failing them.
The numbers are stark. Research published in JAMA and related journals has found that only about 28% of dialysis patients aged 18 to 69 are referred for transplant evaluation within one year of starting dialysis.¹ Among young patients with zero comorbidities, the people who would benefit most, roughly 30% are waitlisted within a year, and just over half within five years.² Referral rates vary dramatically by facility, ranging from nearly zero to over 75%, meaning that a patient’s odds of even hearing about transplantation depend heavily on which dialysis chair they happen to sit in.³
These are not patients failing the system. These are patients being failed by a system that asks them to personally compensate for its own fragmentation.
The kidney transplant pathway is not unique. It is simply a particularly vivid illustration of a dynamic that operates everywhere in healthcare. Cancer care requires coordination across surgery, medical oncology, radiation oncology, pathology, radiology, and often palliative care. Each discipline maintains separate records, separate workflows, separate institutional priorities. The patient moves between them like a traveler without a passport, repeatedly explaining their history, repeatedly discovering that information did not travel with them, repeatedly wondering if anyone is actually in charge.
Chronic disease management, where the majority of healthcare spending actually occurs, is almost entirely a coordination problem. The diabetic patient with comorbid heart disease and depression sees an endocrinologist, a cardiologist, and a psychiatrist, none of whom have reliable visibility into what the others are doing. Medication conflicts go unnoticed. Treatment plans contradict each other. The patient is left to reconcile these contradictions on their own, often without the clinical knowledge to do so safely, often while being blamed for “non-compliance” when the reconciliation fails.
The pattern is consistent across every specialty, every condition, every institution. The more complex the patient, the more specialists involved, the more institutions touched, the worse the information flow becomes. Precisely when coordination matters most, the system is least capable of providing it.
The Economics of Not Getting Better
Now we must ask the uncomfortable question that polite healthcare discourse prefers to avoid. If coordination is so obviously valuable, if better information flow would so clearly improve outcomes, why does the system resist it?
The answer is structural rather than conspiratorial. No one is twirling a mustache in a boardroom, plotting to harm patients. Something worse is happening. The incentives have been arranged such that institutional interests and patient interests quietly diverge, without anyone needing to make an explicitly harmful decision.
A dialysis facility that successfully guides a patient toward transplantation loses a revenue stream. The transplanted patient no longer needs dialysis. From a pure business logic standpoint, the facility has no financial reason to aggressively promote an intervention that ends the patient relationship. CMS requires facilities to “educate” patients about transplant options, but there are no standardized metrics for what this education should contain, no penalties for facilities where referral rates approach zero, no mechanism by which the stated goal is connected to any actual incentive.
Hospitals that control patient records can slow-walk transfers to competing institutions. EHR vendors that make data export difficult benefit from data lock-in as a competitive advantage. Specialists who maintain separate documentation systems create referral dependencies that generate revenue. None of this requires malice. It requires only that institutions act according to their own interests in an environment where those interests are not aligned with patient coordination.
The harm is ambient. It is built into the furniture of the system. The system that is supposed to treat you benefits, in measurable financial terms, from your continued engagement with it. This is the second inversion, and it explains why solutions that have existed for years remain mysteriously unimplemented.
The anthropologist David Graeber observed that bureaucracy is not merely inefficient. It is a form of structural violence. Not physical violence, but the violence of forcing people to navigate arbitrary systems that do not recognize their needs, that demand documentation they cannot produce, that require forms of legibility that erase the complexity of actual human situations. Healthcare bureaucracy is this violence refined to an art form.
When a transplant center requests records from a dialysis facility, or when an oncologist requests imaging from a hospital across town, the request enters a queue. Someone must locate the records, determine what can be released, redact what cannot, prepare documents for transfer. The transfer mechanism is often still a fax machine, a technology from 1964 that remains canonical in American medicine. The fax persists not because it works well, but because it is the lowest common denominator of legal defensibility. Sending a fax is “safe” in a way that digital transfer feels risky to compliance departments, even when the digital option is more secure. The fax may not arrive. If it arrives, it may be illegible. If it is legible, it may be incomplete. If it is complete, it may sit in an inbox for days while someone attends to more pressing matters.
Meanwhile, the patient waits. The clearance expires. The labs go stale. The evaluation window closes. The tumor grows. The heart weakens. The patient is told to restart the process.
The medical literature describes patients who fall out of care pathways as “non-compliant” or “lost to follow-up,” phrases that place the burden of failure squarely on the person who is sick. A more honest description would be that the system lost them. The infrastructure did not exist to carry them through. They were asked to substitute their own exhausted bodies for missing coordination capacity, and eventually they could not.
The record of your care becomes the obstacle to your care. This is the third inversion, and it is perhaps the cruelest.
Truth is the Shortest Path to a Real Solution
There is a certain deep cruelty in asking patients to solve structural problems through individual effort.
“Patient engagement.” “Shared decision-making.” “Health literacy.” The assumption embedded in these phrases is that if we can just educate patients sufficiently, they will navigate the system successfully. This is victim-blaming dressed in the language of empowerment. The patient with end-stage renal disease is not failing to engage. They are engaging with a system structurally designed to resist coordination. The cancer patient is not insufficiently literate. They are trying to read a map that does not exist.
So what would it actually take to resolve the Care Transfer Paradox?
Not better software alone, though better software would help. The fundamental requirement is a reorientation of how we understand health information, followed by governance mechanisms that make the reorientation stick. Currently, health information is treated as institutional property, something to be guarded, controlled, monetized. The patient exists in this framework as a subject about whom data is collected, not as an agent who owns and directs that data. The necessary shift is to reconceive health information as civic infrastructure, shared and patient-directed, with guardrails but without gatekeepers.
Three things would have to change.
First, patient-directed portability with scoped, time-bound consent. Not “release everything forever or release nothing,” but granular delegation. Allow my cardiologist to see my nephrology notes for ninety days. Let this transplant center access my dialysis records until my evaluation is complete. Consent architecture modeled on financial services, where APIs like Plaid manage permissions dynamically, rather than on the all-or-nothing release forms that dominate healthcare.
Second, enforcement mechanisms that change institutional behavior. Voluntary interoperability standards have existed for years and have been voluntarily ignored. Until there are real consequences for data hoarding, whether through reimbursement penalties, regulatory action, or competitive pressure from patients who can actually see which institutions cooperate and which do not, the incentives will continue to favor fragmentation.
Third, workflow-level routing that moves the right information to the right person at the right time. The patient should not have to know which record needs to go where. Intelligent systems, whether AI-powered or simply well-designed, should handle the logistics of care transfer the way logistics companies handle package routing. The patient should experience coordination, not perform it.
None of this is technically difficult. All of it is politically difficult. If the incentives are currently aligned against sharing, as they clearly are, then changing the incentives requires a brute-force intervention. Federal regulation. Changes in reimbursement models that pay for coordination rather than procedures. A willingness to override the institutional risk aversion that currently treats every potential data transfer as a lawsuit waiting to happen.
The patient with kidney disease, or cancer, or heart failure, or any complex chronic condition, should not have to coordinate their own records. The records should follow them automatically, to wherever their care is occurring, with their consent but without their active labor.
The Care Transfer Paradox is not an abstraction. It is a mechanism by which people are harmed every day, in every hospital, in every specialty, in every city.
We have constructed a healthcare system that imposes harm through the refusal to recognize the patient as a coherent whole rather than as a collection of fragmented records distributed across institutions that treat each other as competitors. The sicker the patient becomes, the more fragmented their care. The more fragmented their care, the more valuable their longitudinal data. The more valuable the data, the harder it is to access.
This is the paradox. This is the trap. And the only way out is to stop pretending the problem is technical.
We already have the pipes. What we lack is a system that is rewarded for letting information move.
References
1. Patzer RE, et al. Variation in dialysis facility referral for kidney transplantation among patients with end-stage renal disease in Georgia. JAMA. 2015.
2. Axelrod DA, et al. Rates of solid-organ wait-listing, transplantation, and survival among residents of rural and urban areas. JAMA. 2008.
3. Data on facility-level variation in transplant referral rates from CMS Dialysis Facility Compare and related USRDS analyses.
RELATED ARTICLES
Explore more insights and perspectives from our team.