Why Your Immune System Wasn’t Built for Cities
The evolutionary biology behind the vaccine debate and what a real resolution would actually take
by Serelora
This article was originally published on Medium.
Read full article on Medium
I keep watching grown adults scream at each other over microscopic droplets of science while standing in line at Starbucks. They breathe the same recycled air as forty strangers. They wait for a drink made by someone they will never meet. We have engineered a world where proximity is mandatory. Our kids share classrooms with thirty other immune systems. Rush hour means pressing your face against a stranger’s shoulder for almost an hour. Then we act genuinely shocked when conversations about disease prevention feel personal and explosive.
Strip away the social media theater and the vaccine fight is not really about vaccines. It is about trust. Or more precisely, the rational absence of it. It is about who gets to decide what goes into our bodies when the institutions making those decisions have spent decades demonstrating why they should not be trusted blindly.
Buried underneath all that noise are two questions that actually matter. Questions that neither side likes because the answer indicts everyone.
What if the real problem is not whether vaccines work, but why we have built a world that needs so many of them?
And why the institutions managing that world have made themselves so hard to believe?
The Evolutionary Mismatch We Can’t Undo
For almost the entire history of our species, meeting a stranger was an event. Not a Tuesday. An event.
Anthropologist Robin Dunbar tried to quantify the social capacity of the human brain and landed on a number that has bounced around for years. Roughly one hundred fifty stable relationships. Your band. Your village. Your troop of primates on the savanna. Everyone you would ever know, trust, and swap pathogens with across a lifetime.
Your immune system evolved inside that constraint.
Think about what that really means. The adaptive immune response, that elegant machinery of antibodies and T-cell memory, calibrated itself to a world of sporadic challenge. You met a novel pathogen when your band crossed paths with another band. Maybe a few times a year. Your body mounted a response, recovered, built memory. The long stretches between exposures were not a problem to be solved. They were a feature of the environment. Your immune system expected those gaps the way your lungs expect oxygen.
Now look at what we have done.
In the evolutionary blink of about ten thousand years, we took that organism tuned for occasional encounters in clusters of one hundred fifty and shoved it into subway cars with one hundred fifty strangers. Each of those strangers spent yesterday with a different hundred fifty. Those people are tied to their own networks. The result is a dense mesh of potential transmission that your great-great-grandmother literally could not have imagined.
We invented cities. Then we invented megacities. Places where tens of thousands of people squeeze into every square kilometer. They breathe recycled air through HVAC systems designed for energy efficiency, not immunologic prudence. They touch the same doorknobs, elevator buttons, and coffee counters. Each one a fomite, a polite epidemiological word for object coated in other people’s biology. We send toddlers to daycare, which from a pathogen’s perspective looks a lot like an all you can eat buffet.
Once you see this, the mismatch becomes hard to unsee. We have built an environment that selects for exactly the traits we should fear in pathogens. Viruses that spread quickly thrive. Viruses that mutate rapidly adapt. The density and movement patterns of modern life reward the very characteristics that make diseases hard to control.
Recent outbreaks are not mysteries. They are consequences. When pertussis spikes or measles reappears in urban clusters, it is not because viruses suddenly became more evil. It is because we built habitats that function as amplifiers.
And the part nobody on either side likes to sit with. We are not going back.
The fantasy of minimal touchpoints and tiny self-contained communities is exactly that. Fantasy. Not because the right politician has not arrived yet. Not because we are missing a clever policy tweak. The forces pushing people together are structural.
Jobs, universities, hospitals, airports, logistics hubs, dating pools, cultural life. All of it concentrates in density because that is where efficiency and opportunity live. Migration and immigration are at historic levels. Young people still leave smaller towns for larger ones because that is where the options are. Remote work and rural revitalization exist, but they nibble at the edges of a system whose default setting is interconnection.
So, the honest starting point looks like this. The daycare kid sharing crayons with twenty immune systems. The business traveler breathing airplane air for half a day. The delivery driver touching dozens of doorknobs before lunch. The immigrant family chasing opportunity in a city where opportunity clusters. This is not a glitch that goes away if we complain loud enough. This is the habitat.
Which means the conversation cannot be about returning to some imagined low contact past. It has to be about how you manage disease in a world where high contact is the permanent baseline.
And for that, you have to talk about the people and systems that manage the tools. You have to talk about trust.
Two Truths And The Same Elephant
Before we can move forward, we have to accept something that makes everyone squirm.
Both camps are touching the same elephant. One has a hand on the massive flank and insists it is a wall. The other grips the trunk and swears it is a snake. Each is holding a fragment of truth and insisting that their fragment is the whole thing.
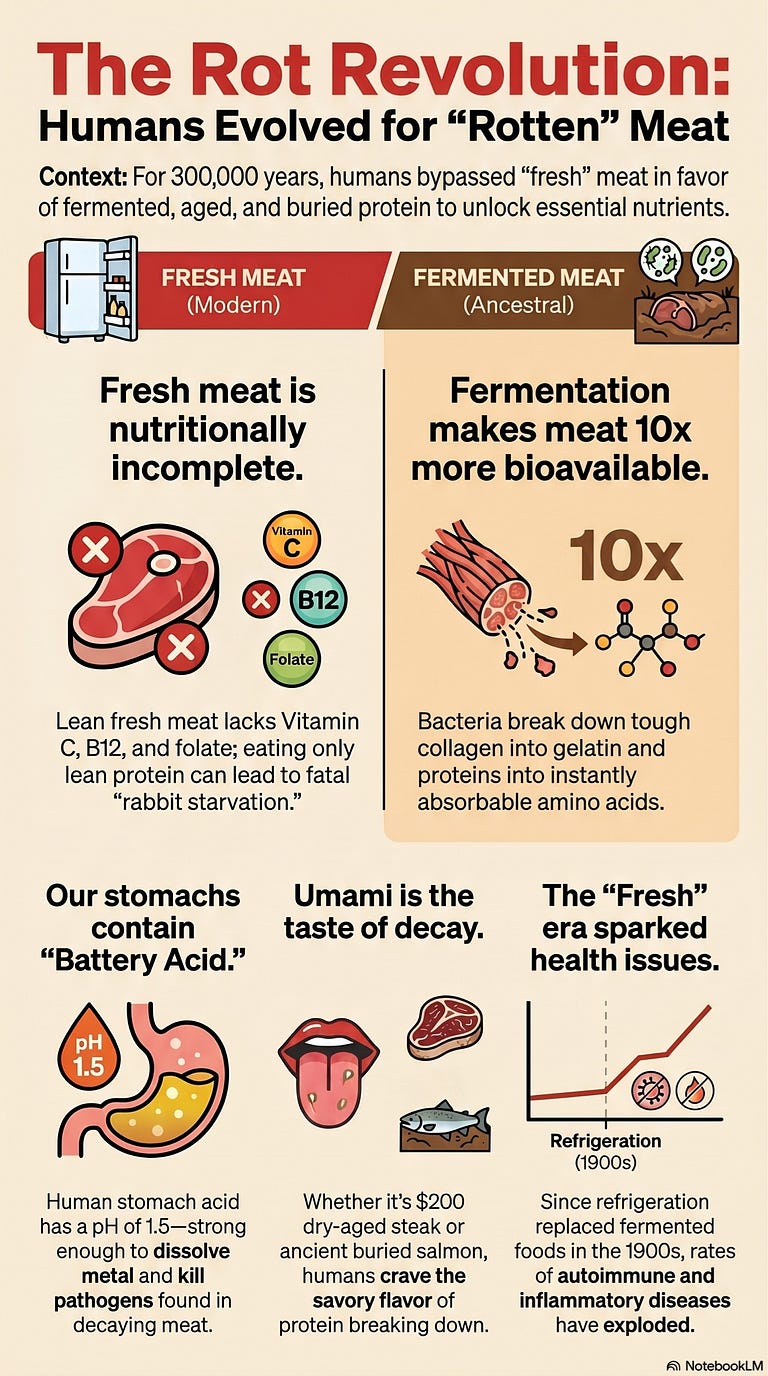
The pro-vaccine world has data. Mountains of it. Smallpox did not vanish because people suddenly ate more kale (although the shift from literally poisonous city food to safer, standardized calories did help, once we stopped killing people with rotten meat, spoiled milk, and canned mystery stew, which is how you end up with cereal empires like Kellogg’s selling digestible breakfast as a kind of industrialized safety blanket). Polio did not retreat because someone installed nicer toilets. If you look at global epidemiology, vaccines have prevented an astonishing number of deaths in the last half century. That is not marketing copy. That is counting.
At the same time, data is not the whole story.
Raymond Obomsawin, an Oneida scholar with a Cornell doctorate in health science and human ecology, spent years digging into historical public health records. What he found was uncomfortable for simple narratives. For several diseases, mortality had already dropped sharply before vaccines arrived. The reasons were boring and powerful at the same time. Cleaner water. Better nutrition. Less crowding. Improvements in basic living conditions that never get a glossy pharma brochure.
His point was not that vaccines are poison. His argument was that we built environments so hostile to human health that we needed aggressive pharmaceutical interventions just to reach a baseline. Then we congratulated ourselves for the interventions and mostly ignored the underlying conditions.
His critics were right that some of his analysis blurred important distinctions, especially between mortality and incidence. Fewer people dying of a disease is not the same thing as fewer people catching it. Vaccines really did crush incidence even where mortality had already fallen. That matters.
Both things can be true. The environment got healthier in ways that saved lives. Vaccines then piled on by reducing the number of infections in the first place.
What gets lost when people dismiss him as a crank is the question underneath his work. Why have we built environments that require such aggressive pharmaceutical intervention just to maintain basic health. And why do we keep building them in ways that intensify the problem.
You cannot answer that without looking directly at the institutions that make decisions about health and risk. Which takes us straight into the trust problem.
Institutions Really Did Earn This Level Of Distrust
The collapse of institutional trust is not a branding issue. It is not a marketing funnel that needs better copy. It is a behavioral problem that institutions created themselves.
The distrust is rational.
The distrust is earned.
The COVID-19 pandemic did not invent this. It just dragged the process of decision making onto the stage while the lights were on.
In early 2020, Anthony Fauci told people on national television that there was no reason for the general public to walk around in masks. Months later he explained that officials had been worried about shortages for healthcare workers. In other words, the guidance was shaped by a real concern and then wrapped in a half truth.
Philosophers call that a noble lie. Deceiving people for their own good. The problem is not just moral. It is strategic. It assumes that ordinary people cannot handle the complexity of reality. Then, when the lie unravels, people stop asking whether something is true and start asking what someone is trying to make them do this time.
Once that frame sets in, every message starts to feel like a tactic.
The mask reversal was only one example. There were others. Sloppy data that lingered in policy longer than it should have. Guidance that moved in ways that seemed synchronized with political timelines rather than clearly grounded in evolving evidence. The lab leak hypothesis declared a hateful conspiracy in one season and a valid scientific question in another, with no serious reckoning for the whiplash. Clinicians who raised nuanced concerns in good faith found themselves deplatformed or labeled dangerous instead of being engaged.
Each incident did not land in a vacuum. They layered. The result was a compound fracture of credibility.
What happened afterwards should trouble everyone. There was almost no visible accountability. No loss of license. No resignations rooted in genuine responsibility. The organizations that demand public trust responded to their own errors with self-protection and quiet spin.
People noticed.
Surveys are not perfect, but they capture the trend. Trust in flagship public health agencies dropped significantly over the span of a few years. Support for routine childhood vaccinations slipped. When researchers asked why, the answers were not about the chemistry of mRNA. They were about confidence in the people making the calls.
One finding should be stapled to every institutional wall. When researchers tested how people respond to honest information about vaccine risks and uncertainties, the pattern was clear. Transparency sometimes reduces short-term willingness. In the long run it builds more durable trust. Manipulation and silence do the opposite.
We could have chosen that path. We did not.
Instead, many institutions embraced a kind of paternalistic messaging. They chose what to say based on what they thought would maximize compliance. Now we are living with the downstream effect. Outbreaks in communities that would likely have vaccinated ten years ago, before the sausage making was this visible.
The way out is not another campaign that says trust us. The way out is to become trustworthy in practice. That means early admission of error. Public accountability. Clear separation between scientific uncertainty and political preference.
Until people see that kind of behavior, skepticism is not a pathology. It is pattern recognition.
Get Serelora’s stories in your inbox Join Medium for free to get updates from this writer.
Enter your email Subscribe
Remember me for faster sign in
That pattern recognition then spills into every related conversation, including the one that generates more heat than almost any other.
The Autism Question Deserves Better Than Slogans
No vaccine issue has produced more emotional shrapnel than autism. Which is remarkable given how clear the evidence is and how badly the conversation has been handled.
If vaccines caused autism in a simple causal way, you would expect a straightforward pattern. Wherever vaccines are given at similar doses and schedules, autism rates would spike in similar ways. Yet we do not see that.
The United States reports autism diagnoses in roughly one child out of every few dozen. Other wealthy countries that use the same vaccines, on similar timelines, often report rates several times lower. When researchers combined data from huge cohorts across multiple countries, they found no association between vaccines and autism.
Natural experiments tell the same story. Japan halted one major combination vaccine for a period. Autism still climbed. Several countries removed thimerosal, a preservative that became a focal point of fear. The diagnosis curves did not bend.
If vaccines were the driver, those shifts would have signaled it loudly. They did not.
That should be the end of the story. It is not, because numbers alone do not address what many parents believe they have seen with their own eyes.
Plenty of parents tell a version of the same story. Their child seemed one way before a vaccine visit and different afterward. Less engaged. Different in a way that felt wrong. They looked for explanations and the timing pointed them toward the shot.
Many of these parents are not foolish or gullible. They are paying close attention to their children. The age when core vaccines are given overlaps with the age when early social and communication differences become noticeable. Correlation is not causation. It is also not automatically irrelevant. It is a clue that needs context, not ridicule.
The context in the United States is peculiar.
Under American law, kids often need a formal diagnosis to unlock services. Speech therapy. Occupational therapy. Support in school. Insurance coverage. The autism label is a key. Many European systems, by contrast, base access to support more on functional need than on a specific code.
American parents are not inventing autism. They are navigating a bureaucracy that will not help their child unless someone checks a particular box. That reality drives more evaluations, more labels, and a much higher official prevalence.
The epidemic is partly real, as criteria have widened and detection has improved. It is partly structural, because the system rewards certain words on paper.
We should be able to hold all of this at the same time. Vaccines are not causing autism. Parents who sense something different in their kids deserve respect and real engagement, not eye rolling. The way we structure access to care in this country inflates labels. The way professionals sometimes dismiss concern pushes families toward communities that validate their fears, even when those communities are wrong about the cause.
Handled well, the autism debate could have been a case study in how to build trust while sharing difficult information. Instead, it became another fracture line.
To fix any of this, you have to understand the skeptics who are reachable without validating the fantasies that are not.
Understanding Skepticism Without Endorsing Fantasy
If you only look at the loudest voices in comment sections, you will miss the real people behind vaccine hesitancy.
Plenty of skeptics look out at the medical system and see a machine that billed them hundreds of dollars for a ten minute visit. They see pharmaceutical companies that aggressively marketed opioids and walked away rich… and only a few incarcerated for purporting the opioid epidemic. They remember experiments like Tuskegee. They’ve watched guidance flip in real time with little to no explanation.
They are not parsing preprints. They are asking a simpler question. Why should I trust you when you have been wrong, harmful, or opaque so many times before.
Surveys back this up. A significant slice of vaccine hesitant adults do not cite scientific doubts at all. They talk about access barriers, bad experiences, and a sense that no one is paying attention to their particular situation. That is not hostility to science. It is hostility to a machine that feels indifferent.
Recognizing the logic of their distrust is important. Confusing that with agreement about solutions is dangerous.
Because there is a hard, non-negotiable reality sitting in the middle of all this. We are not going to unwind interconnection. We are not going to shrink back into little bands with a few dozen exposures across a lifetime. The economic and social architecture of the planet runs on movement, density, and contact.
That means you do not get a version of the future where we simply reduce touchpoints enough to make vaccines optional in any broad sense. You might carve out exceptions and edge cases. You can target schedules and individualize decisions. What you cannot do is pretend that the habitat is going to revert to a low contact default.
Once you accept that, the interesting question shifts. It is no longer vaccines yes or no. It becomes how to use them and other tools in a way that respects individual circumstances, acknowledges real risk, and does not depend on blind obedience to clearly fallible institutions.
That is where viable resolutions live.
What A Real Resolution Would Actually Require
A serious resolution to the vaccine wars is not one change. It is a set of shifts that line up across different levels at the same time.
From institutions, the starting point has to be radical transparency and a different relationship to error. That means saying we do not know when we do not know. It means adjusting guidance in public with the evidence, not quietly editing websites and pretending nothing happened. It means accepting that honest discussion of risks will sometimes reduce uptake in the short term and choosing honesty anyway.
Trust is not a vibe. It is a track record. And part of that track record has to involve confronting the forces that keep leaders from being transparent in the first place.
One of the strongest of those forces is fear of litigation. The whole system is saturated with it. Every hospital executive and public health leader knows there are lawyers circling, waiting for the next case that might turn into a multimillion dollar settlement. That reality makes every admission of uncertainty feel like evidence in a future trial. On the other side, every time a malpractice case turns into a big payout, or a patient and a lawyer squeeze an insurer in a settlement, it reinforces the worst assumption that patients are just trying to cash out. Doctors start to see not only clinical risk but legal risk sitting in front of them. You get a feedback loop where fear of being sued makes institutions more defensive and less transparent, which makes patients more suspicious, which then feeds more litigation and more distrust. You cannot fix that only in courtrooms. You have to change how guidance is made and communicated in the first place.
From public health, we need less one size fits all and more genuine risk stratification for humans, not just populations. The early move toward more shared decision making for some vaccines, where family history and local context actually matter, hints at a saner approach. Not everyone faces the same risk profile. Acknowledging that openly makes people more willing to listen when you say a recommendation really is universal.
From policy and planning, we need to stop pretending that infectious disease is only a medical problem. It is a habitat problem.
Zoning that crams people into poorly ventilated spaces. Labor expectations that punish people for staying home while sick. Transit systems that maximize crowding. Housing and economic policies that make high density the only viable option for millions. All of these shape how easily pathogens move.
We actually have tools to soften some of this. Better ventilation. Sick leave that exists in reality, not just in HR handbooks. Urban design that reduces unnecessary crowding. Support for economically viable life in lower density regions where that makes sense.
None of this erases the need for vaccines. It does reduce the baseline pressure on the system. It is the difference between constantly standing at the edge of a cliff and walking a few meters back.
From everyone, we need an adult level acceptance of the world we actually have.
We live in a permanently interconnected, high contact species level experiment. That is simply true. In that world, vaccines are not optional in any serious sense if we want to avoid mass death and disability. At the same time, institutions do not get to demand trust they have not earned. They have to behave their way into credibility.
The Conversation That Might Lead Us Somewhere Useful
The current vaccine discourse is a stalemate.
One camp shouts about science and demands obedience from people who have watched the scientists’ institutions lie, wobble, and self-protect too many times. The other camp sells an illusion of safety built out of purity and wellness, a package that mixes isolation fantasies where convenient with supplements, detoxes, naturopathic treatments, and spiritual language everywhere else. It feels softer and more human, so people leave a cold clinic, walk into a warm room that smells like lavender, and are handed bottles that are not FDA approved and may be contaminated for all anyone really knows, yet they swallow them because at least someone finally listened.
Neither side is really talking about the elephant. The habitat. The history. The way trust is built and destroyed in real time.
The wellness industry in particular has become an expert at monetizing that broken trust. It tells people they are wise for doubting allopathic medicine and that their intuition beats randomized trials, then quietly steers them toward choices that can be lethal. Women walk away from proven breast cancer therapy to chase juice cleanses, miracle supplements, or ivermectin regimens they saw in a group chat. People with diabetes drop medications that actually control their disease and replace them with cinnamon capsules and wishful thinking. On paper they have escaped Big Pharma. In reality they have simply moved their faith and their money into a different industry that is also lying to them and also treating their body as a revenue stream.
The conversation we actually need starts with some basic honest sentences.
Vaccines really do prevent enormous amounts of suffering and death in a world where humans live tightly packed and constantly mobile. That is reality.
We should still be asking why our built environments and policies keep amplifying disease transmission and what can be done about that upstream.
Institutions really have behaved in ways that justify skepticism. They will not talk their way out of that. They will have to live differently.
Many vaccine skeptics are not ignorant. They are noticing patterns of institutional failure and drawing strong conclusions. Some of those conclusions are wrong about biology. The feelings that produced them are not crazy.
We cannot return to a world of minimal contact, and we also cannot wish away risk by retreating into natural immunity slogans and unregulated powders labeled as wellness. The path forward has to center on making interconnection safer with tools that actually work, not on pretending we can escape risk by hiding in smaller circles or trusting industries that have simply not been caught lying publicly yet.
If we can hold all of those truths in the same frame, the argument changes shape.
It stops being about scoring points on the internet and starts being about the work of building a healthier habitat, more honest institutions, and a culture that can hear complexity without shutting down.
Life turns out to be less about winning the fight and more about navigating complexity with some courage. Less about demanding trust and more about becoming worthy of it. Less about fantasies of going back and more about building something viable on the ground we actually stand on.
That conversation is harder than shouting. It asks more from everyone. It is also the only one with any real chance of leading somewhere worth going.
RELATED ARTICLES
Explore more insights and perspectives from our team.